





The abstract I presented at the 2022 ISSWSH Annual Conference on Can More be Done to Prevent Recurrent Urinary Tract Infections and Uro-genital Atrophy? That was published in The Journal of Sexual Medicine
INTRO: Recurrent urinary tract infections (rUTIs) are a significant problem in women and a burden to the US healthcare system. The frequency of uncomplicated cystitis in young sexually active women in the U.S. is approximately 0.5 episodes per person per year. After a first UTI, roughly 25% of women have a confirmed recurrence within the next 6 months. About 25% of women use hormonal birth control each year in the U.S. and a significant proportion of those women end up experiencing Hormonally Mediated Vulvovaginal Atrophy (HMVA) and other related conditions like rUTI. In some of these women UTIs are sexually induced and present 4-24 hours after sexual activity.
OBJECTIVE: Many patients are either uncomfortable providing symptom information or are unfamiliar with the concomitant nature of HMVA and UTI’s. Many physicians are not professionally trained to recognize rUTI’s may be the result of, or how to recognize, HMVA. I seek to provide a solution to these problems of lack of patient communication and condition recognition by physicians unfamiliar with certain risk factors and symptoms.
METHOD: Following the standard UTI diagnosis and treatment protocol of antibiotics is not a satisfactory outcome for patients. When a repetitive pattern of UTI following sexual activity is acknowledged, prophylactic antibiotics are also an inadequate plan for preventing future UTI’s and not an acceptable quality of life or financially feasible for many. Improving communication to enhance the quality of care by determining if symptoms are due to HMVA, the patient can achieve resolution or improvement of urological symptoms. I believe more can be done to improve communication and future outcomes with little investment such as implementing a survey of 5 simple questions screening for specific criteria.
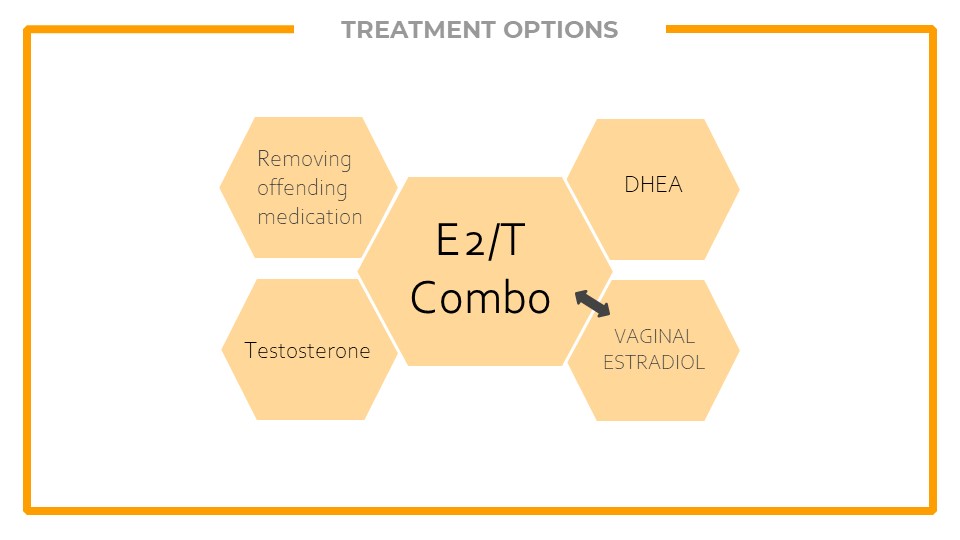
RESULTS: When a broader approach is taken, and questions screening for primary causes of rUTIs are utilized, the correct diagnosis of HMVA or Genito-urinary Syndrome of Menopause (GSM) can be obtained and proper treatment is thus provided to address the underlying HMVA symptoms causing the rUTIs, reducing overall frequency.
CONCLUSION: A brief questionnaire about other urogenital symptoms can be employed to determine if urinary conditions stem from HMVA or if the symptoms are truly only a urological condition. Enhanced communication between patient and HCP can improve the quality of care received and resolve rUTIs much sooner. HCPs have a limited amount of time available to spend with each patient, they do their best to take in patient complaints and determine the best diagnosis and treatment available in time allotted. However, I believe a large proportion of rUTIs and sexually induced UTI can be resolved without much investment from the HCP. A short questionnaire provided to specific patients prior to visit or during visit interview could provide the HCP with important details on the potential source of rUTIs and give direction to the diagnosis and treatment. By screening for signs and risk factors for HMVA, this questionnaire has great potential to improve HMVA and UTI outcomes.

Leave a comment