
A comprehensive article available on how how BV and Yeast infections happen and the role probiotics play in combating these infections!
The original article needed some updates and expansion on some of the info I provided, most of the original info is included in this version so no need to go back and read the original, enjoy!
Chronic or recurrent Bacterial Vaginosis (BV) and Yeast infections are the bane of a woman’s existence and frankly so goddam annoying I’m contemplating swapping my vag out for a newer model with updated software! Is this a thing yet?? (Honestly, the vaginal fluids transplant option can’t come soon enough…) In the meantime, however, we are left do the best we can with what science and witch craftery provides us for solutions.
These infections, whether chronic or occasional, are *usually* the result of these 3 things, sometimes simultaneously:
- Lack of lactobacillus (Data currently shows that the Nitromidazole class of antibiotics: Metronidazole, Tinidazole and Senidazole DO NOT harm lactobacillus)
- Vaginal pH 5.0 of and above in the case of BV infections
- Biofilms
I say *usually* because candida infections can happen for a lot of other reasons besides the above 3 reasons (insert eye roll) as candida is an opportunistic organism; it can mutate to thrive in low pH or high pH, and will seize any opportunity of impaired vaginal immunity.
These pathogens, or bad bacteria and candida, are also becoming more resistant to the standard medications as well as they are getting much better at developing biofilms which protect them from the treatments we have available.
Here is a great graphic from the paper “The Antibiofilm Role of Biotics Family in Vaginal Fungal Infections” that shows the vaginal walls, beneficial bacteria layer, and pathogens and how the breakdown in the beneficial bacteria barrier allows for infections to start:
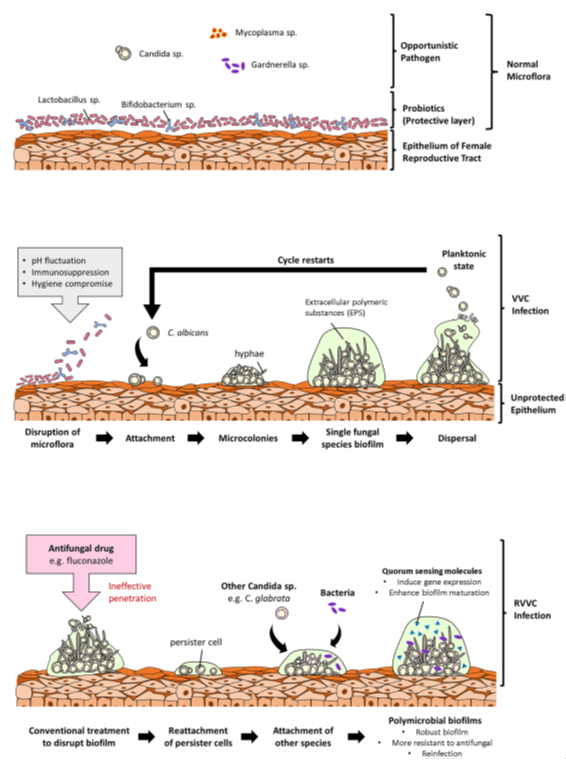
FIGURE 1 | Overview of the role of fungal biofilms in vulvovaginal candidiasis (VVC). (A) Shows a normal vaginal microflora with microorganisms existing cordially. In the normal vaginal microflora, probiotic strains are the primary colonizers, and they confer protection to the vagina by forming a protective layer over the vaginal epithelium. (B) Shows an incidence of vaginal dysbiosis due to unfavorable conditions such as pH fluctuations, immunosuppression, and poor personal hygiene. Opportunistic Candida species then adheres to the vaginal epithelium due to the disruption of the protective layer and forms biofilms leading to VVC. (C) Describes the ineffectuality of commercial antifungals to completely disrupt biofilms leaving behind persister cells. Persister cells of different Candida species can attach to each other or to pathogenic bacteria and form polymicrobial biofilms resulting in a reinfection and RVVC. These polymicrobial biofilms are denser and more difficult for antifungals to penetrate to targeted pathogens. https://www.frontiersin.org/articles/10.3389/fmicb.2022.787119/full#fig1
Next, I will dive into some common reasons that can cause a lack beneficial bacteria, and how an elevated pH can happen. Lastly, I will get into how probiotics are helping and how they are not-because they can have negative effects just like everything else.
There are many causes for vaginal microbiome disruption or lactobacillus/beneficial bacteria depletion, some of the biggies you may or may not be aware of are:
- Hormonal contraceptives. These prevent the production of estrogen, and the synthetic estrogen provided by the contraceptives doesn’t work the same as the type of estrogen our bodies make, so the synthetic type is worthless to you, your vagina, and its microbiome. Without estrogen maturing the vaginal wall cells (called epithelium) to provide a healthy substrate for the lactobacillus to cling to they cannot create a defensive matrix/barrier against pathogens. Estrogen also promotes glycogen in the vagina, which is the food source for the lactobacillus. You may have heard of the Candida diet, while this can be helpful to some it is not a long-term solution-you need glycogen which comes from carbohydrates in your diet. No real estrogen = no glycogen = no food source for the lactobacillus.
- Vaginal penetration with a real-life penis without a condom. Studies haven’t been completed to say with scientific certainty why condomless PIV sex depletes vaginal lactobacillus but there are studies showing it does compared to PIV sex with condoms. You would think any friction against the vaginal walls, condom or not, would cause a disruption to the lactobacilli matrix but I can only report what the data shows; speculation can spark new research but it’s not helpful in the moment.
- Inflammation. Inflammation causes the destruction of epithelial cells lining the vaginal walls and minor tissue sloughing; if left to continue this shedding of the vaginal walls can cause significant loss of beneficial bacteria.
- Profuse shedding of the vaginal epithelium is one of the vagina’s defense mechanisms against a candida or BV problem. Shedding of the vaginal walls is in attempt to prevent candida or BV associated bacteria from attaching, as well as flushing out the canal.
- Antibiotics. Antibiotics don’t just target one type of bacteria, (although this would be a great project for CRISPR, a genetic engineering tool) antibiotics are usually considered ‘broad spectrum’ and some antibiotics kill the beneficial bacteria along with the pathogenic (bad) bacteria. NOTE: Metronidazole/Flagyl and Tinidazole do not harm lactobacillus. Flagyl is the most commonly prescribed antibiotic for BV infections, however, Clindamycin is one of the antibiotics that is harmful to lactobacillus.
- Low estrogen. There are various health conditions and medications (besides hormonal contraceptives) that cause low estrogen and are Google-able so I won’t list them all here, but the biggies are infertility; PCOS; perimenopause/menopause; some antihistamines; and the acne treatment Spironolactone.
- Douching. I know some women insist that this is the only thing that keeps their odor away but that’s like saying spraying a lawn with Round Up keeps the weeds away. Well yeah, but it also keeps the good plant life away too.
- Boric acid OVER USE. I will refer to this again later in the article, but it warrants listing here as well. Boric acid is great-in moderation. Boric acid, which I have a whole separate article on, breaks down the protective biofilm of ALL bacteria and yeasts, this includes the good bacteria. The vagina is constantly breaking down and replenishing the supply of lactobacillus but at a controlled rate. Boric acid speeds up the breakdown process faster than you can replenish the supply. When there is an active infection the use of boric acid every night is beneficial in the grand scheme, but it should not be used more than 1-2 times per week without an active infection present and without consulting a qualified medical professional who has extensive knowledge of these matters, otherwise over use could be depleting your beneficial bacteria defense system.
While a lack of lactobacillus and/or a weakened vaginal immunity can be the causes of BV infections, there are other reasons, such as an elevated pH from menstrual period blood, the natural rise in pH during mid-cycle cervical mucus, etc. Many BV infections can be traced back, in part, to an imbalance in pH levels (regardless of lactobacillus levels) but are ultimately due to the vaginal defense mechanism, in totality, being disrupted. BV flourishes in a pH of 5.0 and above, the preferred range of the vagina (3.5-4.5pH) is too acidic for BVAB to survive. Yeast, on the other hand, is an opportunistic organism and can become problematic in a wide range of pH’s, it doesn’t really care–if the defense system is down, the yeast will multiply and take over. Candida can even CHANGE ITS FORM depending on the vaginal pH in order to adapt and survive! Unfortunately, once one of these infections happens it can be difficult to break the cycle and get back to a place of health and stability.
Something caused the depletion of your vagina’s lactobacillus, and depending on what antibiotic you used for your BV infection, the antibiotic may not be the culprit. It’s more likely that you ended up with a BV infection due to a drop in your lactobacillus amount, leaving your vagina susceptible to BV associated bacteria overgrowth.
In the case of developing a yeast infection after antibiotic use, this is typically due to the void left behind after antibiotic use. The low lactobacillus + no other bacteria competing for nutrients = nothing standing in the way for yeast to multiply uncontrollably.
Just having a menstrual cycle causes the pH to fluctuate so I typically recommend against the use of pH testing strips for this very reason-the vaginal pH fluctuates not only hour to hour, but day to day, week to week, etc. so it’s not a very reliable test. Here are some of the most common causes of elevated pH that doesn’t have to do with lack of beneficial bacteria:
- Cervical mucus, that occurs in the follicular phase and close to ovulation, raises the pH to around 6+ to prevent disrupting sperm mobility
- Sexual arousal and orgasms can temporarily raise the pH simply from flooding the vaginal canal with lubrication
- Menstrual blood (and for some even the hours before blood flow starts) is around 7pH acting as a trigger for some people who menstruate
Originally, I stated there were
“studies showing that taking 10 billion CFU’s of an ORAL probiotic
formulated for vaginal flora including L. Crispatus twice per day for 60 days
and then once daily from then on is having a success rate of reducing recurrent
Bacterial vaginosis infections by 60% and yeast infections by 93%!”
This data is from using the probiotics after a course of antibiotics or antifungals, eliminating the infection, and then an attempt to boost the vaginal microbiome with beneficial bacteria via the intestines or by direct inoculation from vaginal insertions . There are newer treatment protocols for recurrent BV infections-it still recommends taking the probiotics after the course of antibiotics (and the simultaneous start of 21 days of vaginal boric acid). The UpToDate.com recommendations are to use LACTIN-V (which is a L. Crispatus vaginal gel being developed) vaginally, nightly, for 11 weeks but saying “the product is not commercially available, and study results should not be extrapolated to [presume to be the same as] other probiotic remedies.” (However, the other studies I reference did not use LACTIN-V when reporting their benefits but instead they used other oral and/or vaginal probiotic products, so do with that information what you will-I can’t provide medical advice, you must make the most informed decision about your health as you can; weighing both the benefits and the risks of using an oral probiotic inside the vagina and seek the guidance of a well-qualified medical professional who has extensive knowledge in treating recurrent vaginal infections) BUT after all the disclaimer above, the current treatment protocol for BV infections is to insert an L. Crispatus probiotic for 1 1 weeks to boost the amount of lactic acid producing lactobacillus in the vagina.
**Please note that LACTIN-V only contains 2 billion CFU’s of L. Crispatus per application so if you do choose to make your own vaginal insert, there’s no need to use a lot!**
Look for a “women’s” or vaginally formulated probiotic, free of dietary allergens, that contains the following strains: L. crispatus, L. reuteri, L. rhamnosus, L. acidophilus, L. plantarum, L. lactis, L. gasseri, L. paracasei, L. brevis, L. delbrueckii, and Bifidobacterium longum—these strains are “native inhabitants of the female reproductive tract. They often defend the host against fungal colonization through mechanisms such as the secretion of metabolites to inhibit fungal adherence, growth, proliferation, and hypha to biofilm formation” (Fuochi et al., 2019; Wegh et al., 2019 Kalia et al., 2020).
- L. Crispatus is the main strain that produces the bulk of lactic acid and and is most plentiful in the follicular phase.
- Lactic acid is what keeps the pH low
- L. reuteri and L. rhamnosus act very similar to boric acid in that they can break down biofilms; these are most plentiful in the luteal phase, when they usually are most needed. These 2 aren’t the only strains that can perform this act, many of the other’s listed are also biosurfactants which suppress biofilm formation
- L. plantarum helps control the inflammatory process, L. acidophilus helps control the immune system, L. lactis helps in the creation of lactic acid, L. gasseri helps prevent inflammation, L. paracasei promotes epithelial cell growth and mucosal barrier, L. brevis helps increase natural killer cells, L. delbrueckii supports the immune system and helps regulate glucose, Bifidobacterium longum helps reduce inflammation and produces some lactic and acetic acids.
SIDE NOTE: I have another article on Boric acid that you may want to read as well that coincides with probiotic use in helping to stop the cycle of infections. While boric acid can be fatal if swallowed, and must be used cautiously and sparingly, an adult would have to swallow a whole pill worth to cause significant, permanent damage or death.
According to the National Pesticide Information Center:
- Minimum oral lethal doses of boric acid in humans have been estimated from accidental poisonings to be in the range of 500-2000 mg for adults, 300-600 mg for children and <500 mg for infants.
- Acute ingestion of boric acid or borate salts in humans has rarely led to severe toxicity. Commonly reported symptoms include nausea, vomiting (often with blue-green coloration), abdominal pain and diarrhea (which may contain blood or have a blue-green color). Other less commonly reported symptoms include headaches, lethargy, weakness, restlessness, tremors, unconsciousness, respiratory depression, kidney failure, shock and death.14,17,18
- Large oral exposures have resulted in an intense red skin rash within 24 hours of exposure, followed by skin loss in the affected area 1-2 days after the skin coloration first appears. These skin rashes typically affect the face, palms, soles, buttocks and scrotum.17
- Infants ingesting small amounts of boric acid in acute exposures displayed irritability, vomiting, erythema, exfoliation, diarrhea and nervous system affects.11,19 Chronic exposure to borax in infants has led to seizures, vomiting and diarrhea.11
There’s a lot of debate about whether probiotics work or not, and the scientific data is just as undecided. This is due to some research data showing they don’t work and some showing they do. A big part of the discrepancy is due to the study methods, participants, and aggregation of the results.
Let me break this all down:
- Methods. Depending on what product was used; depending if the researchers truly had an idea of what needed to be studied; depending on how much background Science already has on the subject in general or is someone embarking on a whole new concept; what were the end results researchers were looking for when they made their conclusion? There are a lot of variables in the ‘methods’ section alone.
- Participants. A participant may not even need the strain contained in probiotic being tested and if a participant wasn’t deficient in the strain/s being tested, they may not show/report any noticeable changes. They may be on a medication researchers weren’t even aware that could be causing a conflict. Participants can lie-there’s a whole movement of “professional guinea pigs” who live off of the money they receive for participating in clinical trials. Some of these people lie in order to be selected to participate, some lie about effects they have/don’t have, some don’t comply properly with study restrictions, etc. All of these have the potential to skew results.
- Aggregation of results. While aggregation can be useful, it is my opinion, that aggregated data should not be what is conveyed as the most important results of a study. I think that it should be used as a tool to see if something is common but when you aggregate (combine everyone’s data results to provide a summary of what is average/normal) you leave out/dismiss the experience of everyone who didn’t fit into the “average” or “normal” and the number of people who are outliers from “average” can be higher than you think. This all means that there are a lot of people who show great benefit from certain strains of beneficial bacteria probiotics but this data can get dismissed because most of the participants in a particular study didn’t show any changes and conclusions of study results typically report what the most common data showed.
There is hard evidence that, just like with vitamins, the body can only utilize so many CFU’s at once. There is a lot of scientific jargon and concepts behind this but your take away is that 90 billion CFU’s per dose is not going to do anything more or better for you than say 10-25 billion CFU’s per dose and in fact some people can develop bloating, IBS or something called Cytolytic Vaginosis from the over growth of lactobacillus-these people must be careful to not promote this uncontrolled growth of beneficial bacteria. CV is much rarer than what social media will have you believe though and thankfully there is a simple and inexpensive test for it, there’s no need to guess.
Probiotics DO, however, exert their immune related effects on the body as they pass through the digestive/intestinal tract and while inside the vagina. This behavior provides great benefit to many, but I suspect only to those who need the strains they are using or ingesting. If you are not deficient in a certain strain you’re probably not going to notice any effects from taking more of it except maybe a lighter wallet. In other words-they are providing benefit to many who have low lactobacillus/beneficial bacteria and need to replace them.
Lactic Acid producing bacteria strains “are also able to auto-aggregate and co-aggregate to enhance probiotic bacteria adherence on the vaginal mucosa surfaces, and …assist in the formation of biofilm-like barrier that prevents pathogen colonization” (Milik et al., 2013 Mohanty et al., 2019). This means that Lactobacillus are able to create their own matrix and biofilm to create a strong barrier against a bad organism from getting a foot hold. Lactobacillus probiotic bacteria are able to “adhere to the vaginal mucosa…temporarily populating the vagina and creating an environment conducive (helpful) to the restoration of the host’s (endogenous) lactobacilli rather than a return of pathogens.”–(https://www.frontiersin.org/articles/10.3389/fmicb.2022.787119)
Due to a lack of clinical studies and pharmaceutical companies catching on to the need, there is a serious lack of vaginal probiotic products that actually contain the needed strains. This can be a bit of an issue when taking oral probiotics simply due to the time it takes for beneficial bacteria to migrate from the rectum to the perineum skin to the urogenital complex (the vagina and urethra) where they are needed. Many women have resorted to putting their probiotics into veggie capsules that disintegrate easily in the vagina as a way to use an oral probiotic inside their vagina.
Probiotics are great for those who need them, but they aren’t a perfect solution-they really only provide benefit to those who need the particular strains in the product purchased, they aren’t providing long term colonization but instead are providing a crutch until the body (hopefully) repopulates on its own, and probiotics aren’t successful for everyone. Some people continue to develop BV and yeast infections despite using probiotics, not using any medications that deplete estrogen, or performing all of the other recommendations.
Effectiveness can also be the result of a person’s race. Black and Hispanic women naturally have a healthy vaginal microbiome that are not dominated by L. Crispatus which compounds the issue for these women and makes it more difficult to determine which strains to have in the probiotic product.
If you combine probiotic use with the other suggestions from the medical community for prevention such as being extra careful not to spread germs from any anal play to the vagina; not wearing thongs and only wear those all cotton full butt panties and cotton, breathable clothing; getting a re-check to be sure you actually cured your infection; taking stock of any health conditions or medications that could be causing immunity trouble, inflammation, or low estrogen; not using soaps, douches, anything scented; no wipes on the area, only use warm water to clean the vulva; avoid sexual stimulation if the tissues are sore or inflamed; and most importantly- give your body time to HEAL and you should start to see a decrease in the number of infections.
Too many times I have seen online someone asking how long they have to wait to have sex after X treatment, or can they have sex with their partner who’s in town for a holiday vacation after just taking a Diflucan or boric acid? Ladies/Trans Men/People born with vaginas-PLEASE just let your poor vagina heal! I promise you, no matter how aroused you are or how much you/your partner have been looking forward to this intimate time together-your health is more important. If you broke your leg you wouldn’t start training for a marathon until the leg was ready, give your vagina the same consideration, it will be healthier in the long run.
Here is another great graphic from the paper “The Antibiofilm Role of Biotics Family in Vaginal Fungal Infections”:
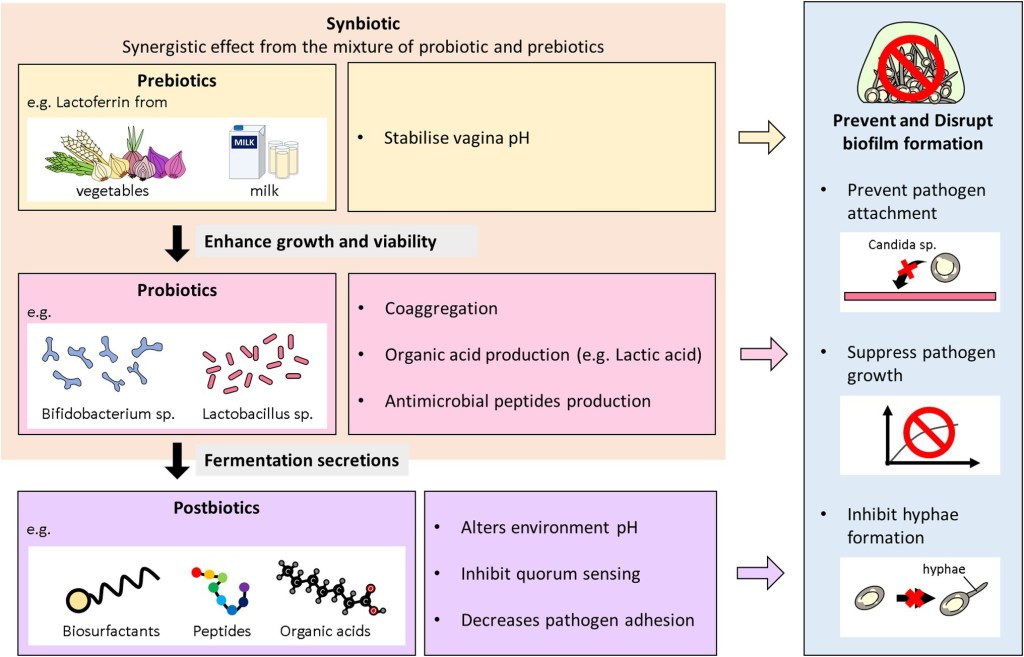
FIGURE 2. Overview of the antibiofilm role of biotics family in VVC. This diagram illustrates the role probiotics, postbiotics, prebiotics, and synbiotics play in preventing and inhibiting biofilms formation of Candida species in VVC infections.
Basically, what this graphic is showing is how prebiotics, probiotics and postbiotics are all playing a role in vaginal (and gut) immunity.
I also want to highly recommend that you:
- Make sure to have confirmation of a yeast infection before you treat with an OTC cream as you can cause crazy irritation or dermatitis to your genitals. Despite the product claiming to be safe for vaginal use, the ingredients in those creams are incredibly irritating to the delicate vulvovaginal flesh.
- Understand that vestibulitis, pelvic floor issues, vestibulodynia, and the start of Lichen Planus or Lichen Sclerosis can feel very much like a yeast infection (and so can vulvovaginal allergies-check out this other article I wrote on that) and treating with creams can make things worse so work with your medical provider to confirm all infections whether BV or yeast and treat accordingly.
- Don’t take antibiotics without a confirmation of an infection. Too many medical providers are prescribing antibiotics for “symptom relief” when it’s the last thing you should be taking. What they don’t realize is most antibiotics, and Diflucan, have strong anti-inflammatory properties to them which makes your delicate bits feel great! temporarily……. but if you didn’t actually have an infection and took an antibiotic unnecessarily you run the risk of making things so much worse.
I also want to reinforce that anyone with a vagina, sexually active or not, can get a BV and yeast infection so these are never something to feel ashamed of for having. I know they can feel uncomfortable and sometimes embarrassing but don’t let anyone cause you to feel abnormal or dirty, the vagina is a delicate ecosystem and can be difficult to maintain especially once the microbiome has been disrupted at least once.
So, get tested, get resistance testing for chronic infections, get the right medication for what ails you by making sure your health care provider checks the UpToDate website, and get to the bottom of what has your vaginal health defenses so low in the first place by seeing a vulvovaginal specialist if needed!
Studies and research data mentioned:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5770522/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2662373/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3720897/
https://www.uptodate.com/contents/bacterial-vaginosis-treatment#H2310740770
https://journals.asm.org/doi/10.1128/mBio.00055-11
https://pubmed.ncbi.nlm.nih.gov/16651720/#:~:text=Abstract,all%20strains%20at%20pH%204.

Leave a comment