
Despite the abundance of readily available and up-to-date clinical data and expert recommendations that doctors have access to during your exam, many clinicians still prescribe outdated and sometimes inaccurate treatments for Bacterial Vaginosis (BV) and yeast infections (YI). Frustrated for effective solutions you turn to the internet, social media, and various Reddit groups to understand why your infections persist or recur. Desperate for relief, you hope to discover a treatment regimen you haven’t yet tried.
Or, you saw a clinician who recommended you take a probiotic during/after your antibiotics because they said “antibiotics kill off the good bacteria” but that didn’t seem to help. They are expensive, there’s not guidance on which one to buy so you buy the ones labeled “women’s formula” only to feel like it didn’t really help.
I wrote a very helpful article on what strains of lactobacillus you should be sure are included in the product you buy based on what study data indicates is the most effective, and how data suggests they should be used for maximum benefit. You can find all of that info here in the article called UPDATE to the Role of Probiotics in Combating BV & Yeast Infections)
You might have seen online that boric acid use is gaining popularity, with many women claiming it helped them finally overcome their infections. Alternatively, a clinician might have suggested boric acid, but again their instructions were unclear—they may not have specified how long to use it or advised using it only after your prescription. Additionally, online discussions can be confusing, with some people stating that boric acid is rat poison or too dangerous to use. (For accurate information on boric acid toxicity, you can refer to what the Poison Control center has published and find recommended instructions and clinical data in this article I wrote called Facts About Boric Acid Treatments.
So you end up trying boric acid and, after a few days, maybe experience irritation or spotting. This can leave you wondering: “Did I do it wrong?” “Is this a sign it’s working or not working?” “Everyone else said it cured their infection; is my infection resistant?” Or, you follow advice and find that your infection or symptoms return the day after stopping boric acid use.
You’ve tried countless rounds of antibiotics or antifungals; you’ve tried months of suppressive diflucan or metrogel; you’ve sent your vaginal swab off to one of those expensive Evvy/Juno/MicrogenDX testing companies that weren’t covered by insurance, only for it to tell you that you still have an infection, or that all pathogens are clear but your microbiome is majorly made up of L. iners. What now?!
**BTW, this article isn’t for those who’s tests come back negative. If you are experiencing symptoms despite negative tests OR symptoms go away while using antibiotics/antifungals but then the symptoms return once the treatment is done and tests still tell you that you are negative for an infection–you almost certainly don’t have an infection, your symptoms need a more in-depth exploration by a specialist. There are many conditions that mimic infections, and ones you wouldn’t necessarily think of, for example a pinched pelvic nerve can cause vulvovaginal itching, burning and excessive discharge. Seasonal allergies can affect the vulva/vagina-the vagina is a mucous membrane just like your eyes and nasal passages and it’s just as susceptible to allergens due to how the body circulates the blood supply.
But for those whose tests keep coming back positive the FIRST thing to do is to verify your pathogen and it’s susceptibility to the medication your clinician is prescribing. Most of the time it is but sometimes, for example, the candida isn’t the “easy” one (candida albicans), sometimes it’s candida glabrata. While resistance is possible among BV and YI, it’s still not that prevalent and most of the time when a cure isn’t achieved it’s due to the prescription’s inability to penetrate the biofilm your pathogen has created. Candida create a biofilm just as BV bacteria do and antibiotics and antifungals CANNOT break through these biofilms to work their effect on the pathogen, the mechanism just isn’t there, the medication is literally unable to do it’s job. Additionally, you may have a candida strain that isn’t susceptible to the medication you keep getting prescribed.
The SECOND thing to do is make sure you are getting the most up to date treatment recommendations by the experts who study these vaginal pathogens and treatments. I know we all naively expect clinicians to provide us with care based on the most recent/updated info but the reality is they don’t and for multiple reasons I won’t get into here, this article is long enough lol.
Sometimes the info is behind a paywall or buried deep in an electronic health records system and the clinician wasn’t given notice that treatment recommendations were updated; so while this info is technically available to everyone, it isn’t the easiest to find unless you know where to look, and what to look for. I’ve made it super simple and easy–Below I describe what the most recent treatment recommendations are based on the latest clinical data, and as always, links to the data and sources are at the end of this article.
You may have tried some of the treatments listed but I can bet that most of you haven’t been told to use the treatments in the following recommended combinations. So long are the days of single treatments being prescribed over and over for chronic/recurrent BV/YI, there is a reason the standard prescription regimens aren’t working, or not working long term, and we are finally starting to figure out why and what to do about it.
“Insanity: Doing the same thing over and over and expecting different results” is drs. prescribing the same Metronidazole or Fluconazole pills for the millionth time without figuring out why the patient still has symptoms and if there is info available to help fix the problem.
Nothing I give you below is any type of new medication, it’s not any unfounded homeopathic treatment–what’s different is that the expert researchers who study and treat these vaginal infections are finding out new combinations of treatments based on what they are recently learning about these pathogens such as the existence of biofilms and the antibiotics’/antifungals’ inability to penetrate through them. Basically, there are updates to treatment protocols and the info isn’t getting utilized by enough clinicians.
NOTE: ALMOST EVERYTHING WRITTEN PAST THIS POINT IS DIRECTLY QUOTED FROM THE RESEARCH ARTICLES AND TREATMENT RECOMMENDATIONS WHERE I FOUND THE INFO. I SUCK AT IN LINE CITATIONS AND SOMETIMES I MUSH INFO FROM MULTIPLE SOURCES TOGETHER TO MAKE IT MORE USEFUL AND COHESIVE FOR YOU. ALL SOURCES OF MY INFO ARE CITED AT THE END OF THIS ARTICLE. No plagiarism intended, only direct to consumer knowledge transfer with little/no changes to the info unless to make it easier to consume.
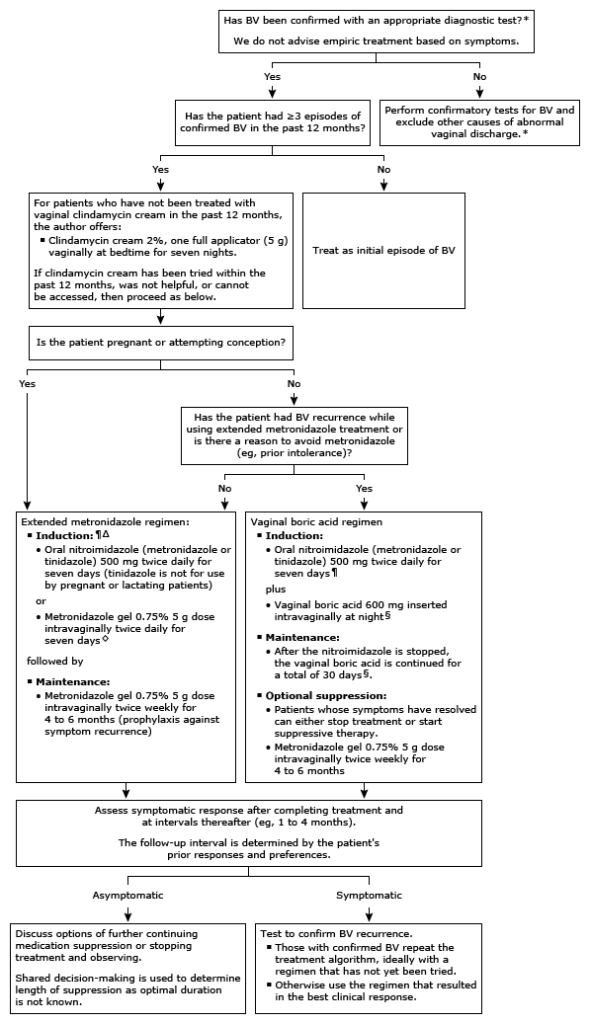
Bacterial Vaginosis (BV) Treatment recommendations–
When possible, treat recurrent BV using a different drug or regimen from what was used from prior therapy given that some patients may have multiple recurrences or recur on maintenance therapy.
- Extended metronidazole only regimen – For patients with recurrent BV, we suggest maintenance intravaginal metronidazole gel after induction nitroimidazole therapy rather than induction therapy alone
- Induction – The choice of oral pill or vaginal gel for induction is based upon patient preferences, prior patient response, and drug availability. Patients often prefer oral to vaginal therapy but both are effective.
- Oral nitroimidazole (metronidazole or tinidazole, 500 mg) twice daily for seven days *If you experience GI upset, try ginger root powder capsules, many find it super helpful.
OR
Intravaginal metronidazole 0.75% gel given as a 5-gram dose twice daily for seven days.
*Here’s the article I wrote detailing how these antibiotics DO NOT harm lactobacillus - Maintenance – Maintenance therapy is started immediately after finishing induction treatment.
- Metronidazole 0.75% gel, 5-gram dose, placed vaginally twice a week for four to six months.
- (We) use maintenance therapy as prophylaxis against symptom recurrence and, in some cases, to increase chance of cure. Patients who remain in remission may elect to continue maintenance therapy for a longer duration. As the optimal duration of maintenance is not known, we use shared decision-making with the patient to determine length of treatment.
- Relapse of infection – Patients with confirmed recurrence that is likely due to relapse, next try the extended vaginal boric acid regimen below.
- Oral nitroimidazole (metronidazole or tinidazole, 500 mg) twice daily for seven days *If you experience GI upset, try ginger root powder capsules, many find it super helpful.
- Induction – The choice of oral pill or vaginal gel for induction is based upon patient preferences, prior patient response, and drug availability. Patients often prefer oral to vaginal therapy but both are effective.
- Extended vaginal boric acid regimen – For this approach, the patient starts an oral nitroimidazole and vaginal boric acid at the same time followed by the option of suppressive treatment with vaginal metronidazole gel for patients who achieve remission. While solo boric acid has been used to reduce vaginal odor, it does not eradicate infection.
- Induction –
- Oral nitroimidazole (either metronidazole or tinidazole, 500 mg, orally twice a day)
PLUS
- Oral nitroimidazole (either metronidazole or tinidazole, 500 mg, orally twice a day)
- Maintenance –
- Vaginal boric acid 600 mg daily (typically at night) for a total of 30 days. After seven days, the nitroimidazole (antibiotic) is stopped while the vaginal boric acid is continued for a total of 30 days. Boric acid should never be used orally.
- Induction –
- Suppression – Patients who achieve remission based on Amsel criteria or similar have the options of stopping treatment or immediately beginning metronidazole 0.75% gel, 5 gram vaginally twice weekly for four to six months as suppressive therapy. The decision to start suppression is based on shared decision-making with the patient.
- Reassessment – One to two days after finishing the vaginal boric acid, patients are evaluated for evidence of remission based on Amsel criteria or similar.
*Remission – Those who achieve remission have the options of stopping treatment or continuing with maintenance therapy.
*No remission – Patients who do not achieve remission are retested to confirm BV, evaluated for likely cause of infection and treated again, preferably with a different regimen. If remission is achieved with re-treatment, maintenance therapy is advised to suppress symptoms.
*Obtaining boric acid — Boric acid vaginal suppositories use can be prescribed through a compounding pharmacy or purchased over-the-counter.
*Post treatment lactobacillus support — Lactobacillus crispatus — studies using vaginal L. crispatus for 11 weeks after patient finished a 7-day course of antibiotics was shown to be promising and no serious adverse events were reported. Study data is still inconclusive (some studies show great results, some do not depending on route, dose, etc. used in study) but since BV is most commonly the result of a depletion of vaginal lactobacillus, current recommendations are to supplement with a vagina L. crispatus for 11-12 weeks.
Many have asked when to start the vaginal probiotic especially if they are using Metrogel. New recommendations suggest starting the probiotic right after the antibiotic (both oral and vaginal) so this would indicate that you would insert the vaginal L. Crispatus probiotic opposite the vaginal boric acid (so 12 hrs apart) after the antibiotics are finished. Then, once the 30 days of boric acid is done you can choose to insert the vaginal probiotic at night time if you’d like.
Yeast infection Treatment recommendations –
So many aren’t getting sufficiently tested for candida, especially when you have unresolved symptoms. Here is a quick note on how to get sufficiently tested:
When possible Saline and KOH wet prep microscopy should be performed in all symptomatic females. Reports describing the errors in cases of misdiagnosis often cite failure to perform wet prep microscopy as the most frequently found reason for the error. The need for the use of KOH can usually be overcome if phase contract microscopy is used. A patient with a wet prep finding of hyphae and pseudohyphae, indicative of active growth of C. albicans, does not require additional testing. Only in the instance of persistent infection should yeast culture and susceptibility testing be considered.
In symptomatic patients with negative wet prep microscopy yeast, culture should be performed. Culture also yields valuable information on species other than C. albicans, especially in cases of RVVC where non-albicans species are more frequently encountered. Nucleic acid amplification tests (NAAT) have come into use due, in part, to ease of use in a busy practice. NAAT typically – with individual test variation – provide combined analysis for BV, C. albicans and a few non-albicans Candida, and Trichomonas vaginalis. The high sensitivity of NAAT is an advantage for detecting trichomonas, an alternative cuase of inflammation in the differential. Sensitivity is valuable in detecting a very small Candida spp. Load in patients with RVVC who have become hypersensitive to a small number of yeast. Unlike wet prep microscopy, NAAT cannot provide information on inflammation. In many settings. Wet prep microscopy is recommended first in every case of suspected VVC.
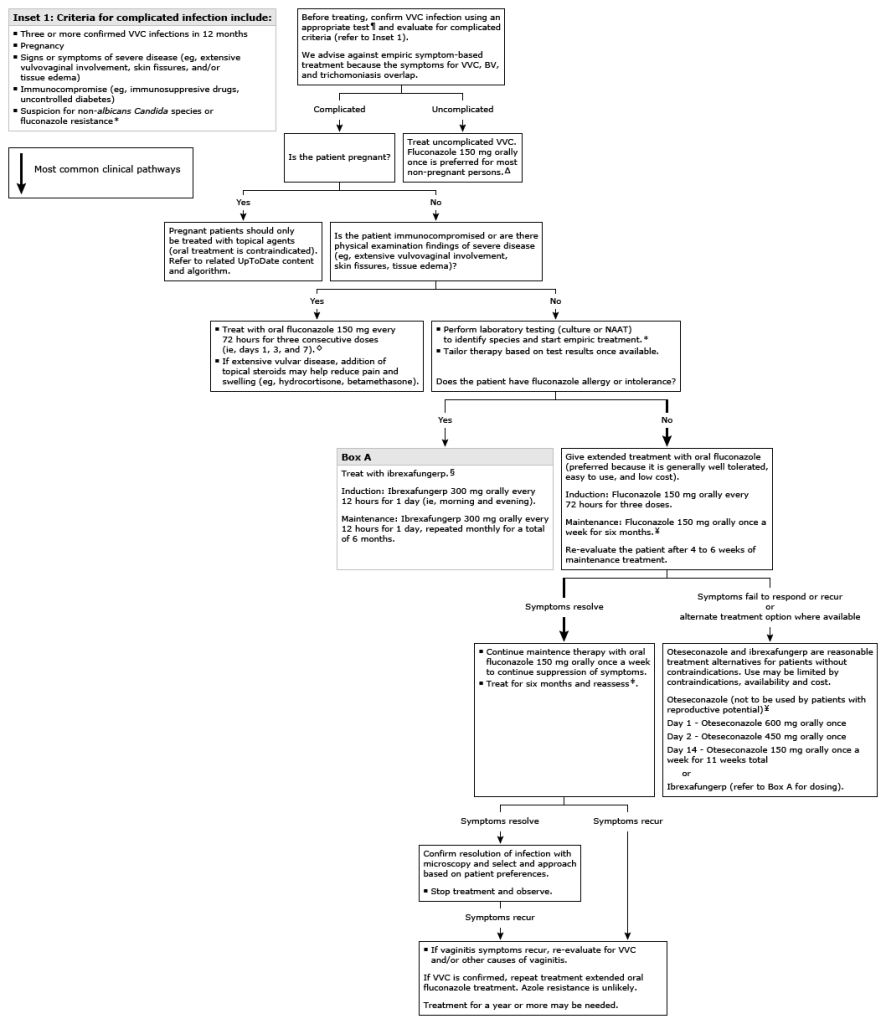
Uncomplicated VVC (vulvovaginal candidiasis) is usually treated effectively with azole antifungal creams, ovules or a single oral fluconazaole 150 mg tablet. An alternative is ibrexafungerp (Brexafemme), the recommended 1-day treatment is 2 tablets (300mg) and a repeated 2 tablets 12 hours later.
In unresponsive cases it is essential to first re-establish the diagnosis, including repeat fungal culture with antifungal susceptibility testing as continuation of symptoms with a negative yeast culture or NAAT may indicate something is happening other than infection such as an irritant or allergic contact dermatitis, hypersensitivity reaction (sometimes referred to as a candida “allergy”) cytolytic vaginosis, neurodermatitis, lichenoid dermatoses, trichomoniasis, desquamative inflammatory vaginitis, pre-cancers/cancers are all conditions that could be causing the initial, or continuation of, symptoms.
Complicated VVC which can be described as primary and secondary:
- Primary is an infection that arises spontaneously with no predisposing biomedical conditions associated with onset or recurrences such as an immunocompromising health condition.
- Secondary is due to an association with immune compromise condition, uncontrolled diabetes, frequent/prolonged antibiotic administration or some other factor such as hypersensitivity to candida antigens (candida “allergy”) as evidence has accumulated linking or defining as association of recurrent vulvovaginal candidiasis with vaginal mucosal immune hyper-reactivity to the fungus, this suggests the occurrence of dysregulated immune reactivity. The likelihood of non-albicans Candida and fluconazole-resistant Candida is greater is why is it essential to to retest and establish if infection is indeed present and that it is sensitive to treatment.
Multiple genetic components have also been identified in conjunction with RVVC and more are likely to be found. Here are those currently identified:
- Bacterial vaginosis- the inflammation caused by BV is a risk factor for yeast infection.
- Mannose-binding lectin (MBL)- the prevalence of a variant of the MBL gene seems to be higher in patients with RVVC than in controls without candidiasis. Impairment of this gene appears to predispose MBL-deficient individuals to recurrent vulvovaginal candidal infections. **This is may why some people are able to find symptom resolution with D-Mannose when all else fails.
- Interleukin-4 (IL-4)- a protein involved in the inflammation process. Those affected by recurrent vulvovaginal candidiasis have a strong inflammatory response when exposed to just small amount of candida, whereas others do not. Elevated IL-4 levels result in the inhibition of the local defense mechanisms that would otherwise limit symptoms and the ability of pathogens to get a foothold. People with elevated IL-4 issues are literally having symptoms with tiny amounts of candida which may not be enough to trigger a positive test result. I still strongly urge you to not just assume this is your issue even if diflucan reduces your symptoms, diflucan has strong anti-inflammatory properties so it could simply be the diflucan suppressing symptoms instead of treating the underlying condition causing them.
INITIAL DRUG TREATMENT Nonpregnant people
- Fluconazole –
- Induction
- Fluconazole, 150 mg, orally every 72 hours for three doses followed by
- Fluconazole, 150 mg, orally every 72 hours for three doses followed by
- Maintenance
- Fluconazole, 150 mg, orally once per week for six month. The role of maintenance therapy is suppression of symptoms and not eradication of organisms. (Probably due to the anti-inflammatory properties of this medication.)
- Fluconazole, 150 mg, orally once per week for six month. The role of maintenance therapy is suppression of symptoms and not eradication of organisms. (Probably due to the anti-inflammatory properties of this medication.)
- Induction
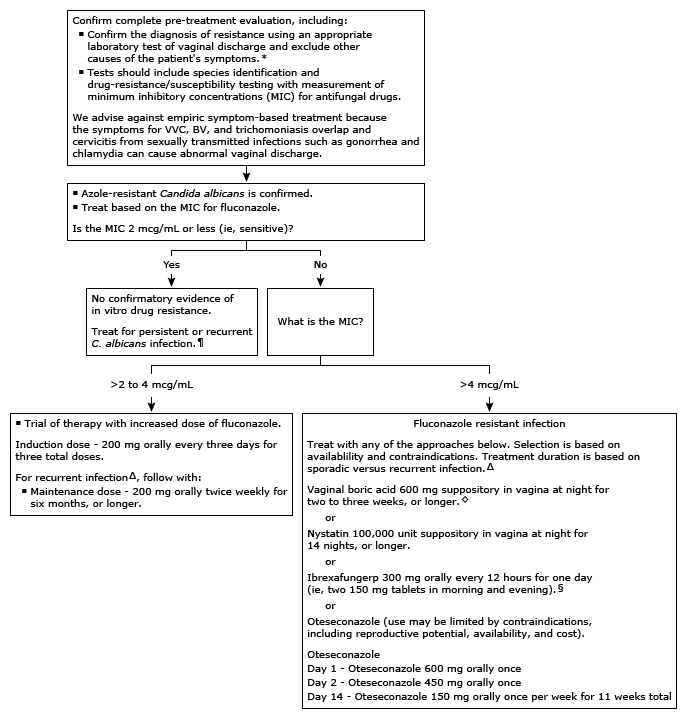
- Oteseconazole -This agent is more potent against Candida species, including Candida glabrata, compared with fluconazole.
Restrictions: Oteseconazole use is valuable but limited only to patients who are postmenopausal, have undergone bilateral tubal ligation, or have undergone hysterectomy. It should not be used in patients of reproductive potential, including those who could become pregnant, are pregnant, or are lactating. Concerns for embryo-fetal toxicity are based on rat studies that reported retinal abnormalities in offspring and because of the long half-life (138 days) of the drug
- Induction for single drug regimen
- Oteseconazole 600 mg orally on day 1, oteseconazole 450 mg orally on day 2
- Oteseconazole 600 mg orally on day 1, oteseconazole 450 mg orally on day 2
- Maintenance
- starting on day 14, oteseconazole 150 mg orally once a week for 11 weeks (ie, once a week dosing during weeks 2 through 12) The regimen is available in a blister pack that indicates the dose and timing
OR
- starting on day 14, oteseconazole 150 mg orally once a week for 11 weeks (ie, once a week dosing during weeks 2 through 12) The regimen is available in a blister pack that indicates the dose and timing
- Induction for dual-drug regimen
- The dual-drug regimen involves initial induction treatment with fluconazole followed by
- The dual-drug regimen involves initial induction treatment with fluconazole followed by
- Maintenance suppression dosing is as follows
- Day 1, day 4, and day 7: Fluconazole 150 mg orally
- Days 14 through 20: Oteseconazole 150 mg orally once daily for 7 days
- Beginning on day 28: Oteseconazole 150 mg orally once a week (ie, every 7 days) for 11 weeks (ie, weeks 4 through 14)
- Induction for single drug regimen
- Ibrexafungerp – Extended treatment with ibrexafungerp, an oral triterpenoid drug, is an option for suppression of RVVC for patients who have not responded to azoles, not tolerated azoles, or have an azole-resistant infection.
- Induction
- Ibrexafungerp 300 mg orally (two 150 mg tablets) taken approximately 12 hours apart (ie, 300 mg taken in the morning and again in the evening)
- Ibrexafungerp 300 mg orally (two 150 mg tablets) taken approximately 12 hours apart (ie, 300 mg taken in the morning and again in the evening)
- Maintenance
- Ibrexafungerp 300 mg orally (two 150 mg tablets) taken twice in one day is repeated every four weeks for a total of six dosing days (ie, extended treatment for six months)
- Ibrexafungerp 300 mg orally (two 150 mg tablets) taken twice in one day is repeated every four weeks for a total of six dosing days (ie, extended treatment for six months)
- Induction
*Pregnant — For pregnant persons with test-confirmed RVVC, we treat with extended courses of topical azoles only. Patients require both induction and maintenance suppressive treatment. Longer courses of induction therapy followed by maintenance for the duration of pregnancy may be required to adequately suppress symptoms. Patients are reassessed after delivery.
- Clotrimazole 1% cream
- Induction
- 1 applicatorful (approximately 5 g) in vagina daily for 7 to 14 days
- 1 applicatorful (approximately 5 g) in vagina daily for 7 to 14 days
- Maintenance
- 1 applicatorful (approximately 5 g) in vagina two to three times a week for duration of pregnancy
- 1 applicatorful (approximately 5 g) in vagina two to three times a week for duration of pregnancy
- (Clotrimazole 2% cream is also reasonable. At this dose, duration of induction therapy is three to five days, as needed to control symptoms. This is followed by maintenance at a frequency that controls symptoms.)
OR
- Induction
- Miconazole 2% cream
- Induction
- 1 applicatorful (approximately 5 g) in vagina daily for 7 to 14 days
- 1 applicatorful (approximately 5 g) in vagina daily for 7 to 14 days
- Maintenance
- 1 applicatorful (approximately 5 g) in vagina two to three times a week
OR
- 1 applicatorful (approximately 5 g) in vagina two to three times a week
- Induction
- Miconazole 1200 mg suppository in vagina once weekly for duration of pregnancy
OR - Miconazole 4% cream and high-dose suppository.
- Induction
- miconazole 4% cream is given daily for three to five days, as needed to control symptoms.
- Maintenance
- miconazole 4% cream at a frequency that controls symptoms (typically 1 to 3 times a week).
OR
- miconazole 4% cream at a frequency that controls symptoms (typically 1 to 3 times a week).
- Induction
- Alternately, miconazole 1200 mg vaginal suppository can be used once a week for the duration of the pregnancy.
OR - Nystatin suppository 100,000 units (may require preparation by a compounding pharmacy).
- Induction
- One suppository in vagina for 14 nights
- One suppository in vagina for 14 nights
- Maintenance
- Vaginal suppository use is slowly tapered to the lowest frequency that controls the patient’s symptoms. Patients whose symptoms are controlled on the nightly regimen reduce frequency to every other night for several weeks. If symptoms remain controlled, the frequency is reduced again to two to three times a week. If symptoms worsen at any point, the patient returns to the frequency that controlled symptoms. Treatment is continued for the duration of pregnancy.
- Vaginal suppository use is slowly tapered to the lowest frequency that controls the patient’s symptoms. Patients whose symptoms are controlled on the nightly regimen reduce frequency to every other night for several weeks. If symptoms remain controlled, the frequency is reduced again to two to three times a week. If symptoms worsen at any point, the patient returns to the frequency that controlled symptoms. Treatment is continued for the duration of pregnancy.
- Induction
- • Vaginal boric acid –Current data suggests vaginal boric acid is used for a limited set of patients, including those with azole-resistant C. albicans, intolerance or allergy to azoles, or non-albicans Candida. Also, current data suggests there is no role for vaginal boric acid or probiotics in treatment of RVVC to usual C. albicans, this is due to data indicating that RVVC is not due to a lack of beneficial lactobacillus. This does not mean boric acid or probiotics won’t help, this statement simply means that current data from studies with a whole bunch of confounding factors isn’t showing reliable enough data to make it a proper treatment recommendation for the treatment of recurrent yeast infections.
- Induction
- Vaginal boric acid (600 mg suppositories) daily for two to three weeks
- Vaginal boric acid (600 mg suppositories) daily for two to three weeks
- Maintenance
- Vaginal boric acid (600 mg suppositories daily) for two to three months. The patient then slowly titrates down the dose. As data-supported regimens are lacking, we have the patient reduce the frequency gradually. Patients who do well with several months of daily vaginal boric acid then reduce to every other day for a few weeks, then once a week for a few weeks, and then stop. If symptoms recur, the process is repeated and the patient maintained on the lowest frequency of vaginal boric acid that suppressed symptoms.
- Vaginal boric acid (600 mg suppositories daily) for two to three months. The patient then slowly titrates down the dose. As data-supported regimens are lacking, we have the patient reduce the frequency gradually. Patients who do well with several months of daily vaginal boric acid then reduce to every other day for a few weeks, then once a week for a few weeks, and then stop. If symptoms recur, the process is repeated and the patient maintained on the lowest frequency of vaginal boric acid that suppressed symptoms.
- Induction
- Gentian violet – Topical gentian violet was widely used prior to the availability of the topical azole intravaginal antifungal creams and suppositories. This agent has largely been abandoned because azole antimycotics are more effective (potent) and because gentian violet is messy and inconvenient (eg, it permanently stains clothes). However, it is useful to treat vulvar itching and for occasional refractory cases of vulvovaginal candidiasis, especially those demonstrating azole resistance.
- The drug is applied to affected areas of both the vulva and vagina daily for 10 to 14 days.
- The drug is applied to affected areas of both the vulva and vagina daily for 10 to 14 days.
- Vaginal nystatin – Vaginal nystatin may be used as an alternative to vaginal boric acid. Dosage is 100,000 units daily (as a pessary or suppository).
- Induction
- Vaginal nystatin is given nightly for 14 nights for induction treatment.
- Vaginal nystatin is given nightly for 14 nights for induction treatment.
- Maintenance
- Patients with recurrent infection require maintenance therapy for six months or more. Dosing for all patients is the same as for pregnant persons.
- Patients with recurrent infection require maintenance therapy for six months or more. Dosing for all patients is the same as for pregnant persons.
- Induction
For patients with intense external burning/itching, triamcinalone 0.1% or betamethasone 0.1% in ointment form can be applied 1-2 times a day until external symptoms resolve.
PLEASE PLEASE BE SURE THAT IF YOU ARE PRESCRIBED BETAMETHASONE THAT IT IS THE 0.1% PREPARATION. BETAMETHASONE IS AVAILABLE IN MULTIPLE STRENGTHS AND IT IS EXTREMELY COMMON FOR DRS TO PRESCRIBE THE WRONG STRENGTH WHICH WILL ONLY BE PROBLEMATIC FOR YOUR VULVAR FLESH AND SYMPTOMS!!
Having chronic or recurrent infections or symptoms that won’t go away is terrible to experience and I’m sorry you have suffered; I’ve been there, and I know that after looking over what the experts recommend you do that it looks long and daunting but isn’t living with an unresolved infection worse? The itching, soreness, odor making you self conscious, the inability to be intimate, the constant anxiety and worry that the infection is back just causing you PTSD or medical anxiety that can take years to get rid of; the bills, upset stomachs, the crying and despair of just wanting to feel like you are functioning normally…….What’s 12 more weeks if the updated treatment recommendations work for you?
Urogenital health depends on many factors. Some additional things to consider that might be at play:
- Drug intake
- Metabolic or immune disorders
- Lactoferrin regulation
- Iron levels
- Steroids
- Chronic inflammatory illnesses
- Certain diseases
- Surgeries
- Cigarettes and alcohol
- Oral microbiota
- Stress has been found to be an actual risk factor for BV infections. This seems a little more abstract but stress triggers a whole set of chemicals and actions that are of benefit to the BV bacteria and harmful to lactobacillus. We live in a world where stress is all too common and chronic infections only add to it but stress can literally be the cause of an infection and chronic infections.
BV is a risk factor for STI’s including HPV but it works both ways. HPV causes certain dysfunctions to the cervical and vaginal tissues putting them at high risk for pathogenic organism colonization. - Hormone equilibrium such as without sufficient estrogen:
- L. Crispatus also will not be able to colonize the vaginal environment and create needed lactic acid if sufficient estrogen isn’t getting to the tissues.
- There’s no recruitment of glycogen for food the lactobacilus starves; vaginal epithelium cells do not mature, and they shed faster than are supposed to-this expedited shedding takes the beneficial bacteria with it as in this scenario they haven’t have enough time to bury into the deeper layers and create their own cellular matrix.
- Epithelial cells don’t mature, aren’t plump and this leaves gaps in the cellular matrix making it very easy for pathogens to bury into the layers, making them incredibly difficult to eradicate.
- Without sufficient estrogen, testosterone, health nutrients from diet/water intake, sleep, exercise and low stress, the vaginal mucous is in short supply, this mucous provides a medium for all kinds of proper mechanisms and provides a barrier against micro abrasions from vaginal penetration, proper flow of various mechanisms, proteins and other components between the vaginal epithelium layers.
Knowledge is power, knowledge gives us tools to combat problems so stay vigilant, keep learning, share evidence based information. Keep finding ways to relieve your stress and see that there is an end to what you are going through-it will give you the strength and energy to push on and to find ways to stay informed-just like you did when you found this article.
Vulvovaginal research and updated treatments and recommendations takes time, lots of it, because vaginal infections are incredibly complex but medical and scientific communities continue to improve on seeing the value in investing in this research.
Please let me know if you have any questions, I am here to help!
Here are the treatment algorithms that were included in the original sources
Bacterial Vaginosis treatment of recurrent infection:
Vulvovaginal Candidiasis treatment of azole-resistant Candida albicans:
Vulvovaginal Candidiasis treatment complicated including recurrent infection of adults non-pregnant:
Vulvovaginal Candidiasis treatment of recurrent infection in pregnancy:

Resources:

Leave a reply to Anonymous Cancel reply